It is well known that aspirin can inhibit the aggregation of platelets and reduce the risk of certain cancers such as colorectal cancer, thus the commonly prescribed recommendation of 81mg baby aspirin (one quarter the dose of 325 mg adult aspirin). This Lancet study explored the one-dose-fits all approach and the theory that this model yields only modest benefits because of underdosing for patients with large-body size and overdosing for patients with smaller-body size. After reading this study, you may reconsider the aspirin dosage for many of your patients.
Aspirin Study Methods
Using individual patient data, researchers analyzed the modifying effects of bodyweight (10 kg bands) and height (10 cm bands) on the effects of low doses (≤100 mg) and higher doses (300–325 mg or ≥500 mg) of aspirin in randomized trials of aspirin in primary prevention of cardiovascular events. They stratified the findings by age, sex, and vascular risk factors, and validated them in trials of aspirin in secondary prevention of stroke. Additionally, they assessed whether any weight or height dependence was evident for the effect of aspirin on 20-year risk of colorectal cancer or any in-trial cancer.ResultsAmong ten eligible trials of aspirin in primary prevention (including 117, 279 participants), bodyweight varied four-fold and trial median weight ranged from 60·0 kg to 81·2 kg (p<0·0001). See Fig. 4, 5, 6 below.
- The ability of 75–100 mg aspirin to reduce cardiovascular events decreased with increasing weight (p weighing 50–69 kg (hazard ratio [HR] 0·75 [95% CI 0·65–0·85]),
- but not in those weighing 70 kg or more (0·95 [0·86–1·04]; 1·09 [0·93–1·29] for vascular death).
- Furthermore, the case fatality of a first cardiovascular event was increased by low-dose aspirin in people weighing 70 kg or more (odds ratio 1·33 [95% CI 1·08–1·64], p=0·0082).
- Higher doses of aspirin (≥325 mg) had the opposite interaction with bodyweight (difference preducing cardiovascular events only at higher weight (pinteraction=0·017).
- Findings were similar in men and women, in people with diabetes, in trials of aspirin in secondary prevention, and in relation to height (pinteraction=0·0025 for cardiovascular events).
- Aspirin-mediated reductions in long-term risk of colorectal cancer were also weight dependent (p was increased by aspirin in people at low weight for dose (p interaction=0·0018) and risk of all-cause death was increased in people weighing less than 50 kg who were receiving 75–100 mg aspirin (HR 1·52 [95% CI 1·04–2·21], p=0·031).
- In participants aged 70 years or older, the 3-year risk of cancer was also increased by aspirin (1·20 [1·03–1·47], p=0·02), particularly in those weighing less than 70 kg (1·31 [1·07–1·61], p=0·009) and consequently in women (1·44 [1·11–1·87], p=0·0069).
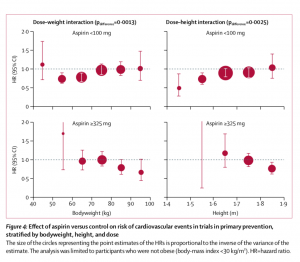
Fig. 5, Click here or on image to enlarge 
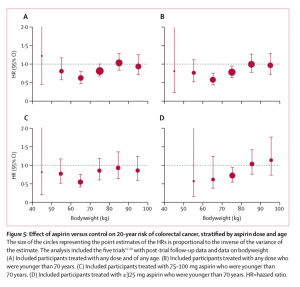
Fig. 6, Click here or on image to enlarge

Interpretation
In conclusion, the optimal dose of aspirin to prevent cardiovascular events depends on bodyweight, driven more by lean body mass and height than by BMI. Low- dose (75–100 mg) aspirin once a day was ineffective in people weighing 70 kg or more, particularly in those who smoked or were treated with enteric-coated formulations, whereas higher doses became more effective with increasing weight. Given that the effects on sudden cardiac death and cancer also showed dose–weight interactions, the one-dose-fits-all strategy for daily aspirin use is unlikely to be optimal.
Low doses of aspirin (75–100 mg) were only effective in preventing vascular events in patients weighing less than 70 kg, and had no benefit in the 80% of men and nearly 50% of all women weighing 70 kg or more. By contrast, higher doses of aspirin were only effective in patients weighing 70 kg or more. Given that aspirin’s effects on other outcomes, including cancer, also showed interactions with body size, a one-dose-fits-all approach to aspirin is unlikely to be optimal, and a more tailored strategy is required.