Seven science-backed interventions to tame inflammation, lower cholesterol, minimize cardiometabolic risk factors and support your patients’ heart health
Of all the disease and conditions practitioners face, cardiovascular health is one of the most complex and nuanced, influenced by factors ranging from gut health to genetics, an effective protocol requires a targeted, highly individualized approach.
“Precision and personalized cardiovascular medicine must be the new medicine of today and the future,” says Mark Houston, MD, Director of the Hypertension Institute. “This means every patient must have a complete genetic profile, a detailed medical history and a comprehensive physical examination, along with advanced cardiovascular labs and testing.”
In addition to a thorough evaluation, personalized protocols should include proven diet and lifestyle therapies shown to address various aspects of cardiovascular wellness, as well as effective, evidence-based nutraceuticals tailored to each patient’s specific needs. Seven science-backed interventions to tame inflammation, balance blood pressure, improve lipid profiles and promote overall heart health.
The right nutrition: Keto, gut health and meal timing.
Studies demonstrate the cardioprotective potential of a low-carb Keto diet. Slashing carbs influences a range of cardiovascular risk factors, including modulating inflammation, normalizing blood pressure, improving vascular endothelium function and benefiting lipid profiles. Compared to other dietary models, the Keto diet appears to be superior to in the prevention and treatment of cardiovascular diseases.1, 2
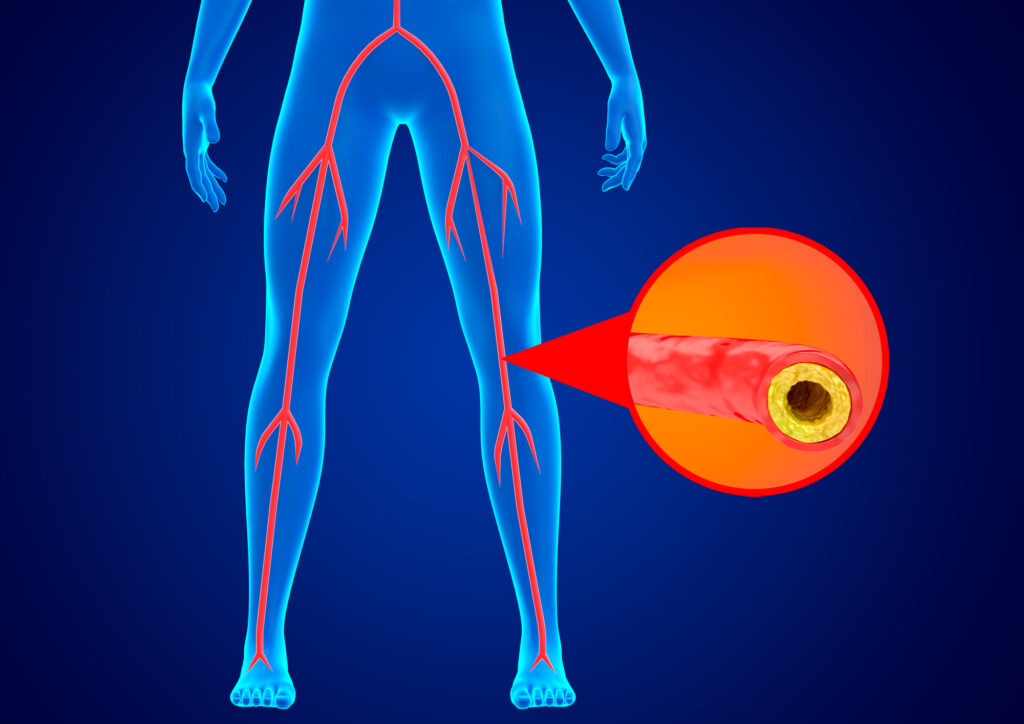
In addition to lessening cardiovascular risk factors, the Keto diet also supports the gut microbiome. Dysbiosis is linked with the development of pathologies such as atherosclerosis, hypertension and heart failure, and recent research suggests favorable changes in certain bacteria may protect against heart disease. The metabolic potential of gut microbiota is a contributing factor: bioactive compounds generated by gut bacteria impact physiology, disrupting blood lipids and activating inflammatory pathways involved in the development of atherosclerosis. The Keto diet appears to have a positive influence on microbiome health, enhancing microbiota diversity, and reducing microbes associated with cardiac events like stroke, coronary artery disease and heart attack.3, 4, 5, 6, 7
Specific dietary components are only part of the picture: the timing of meals may play a key role in cardiovascular health. Intermittent fasting is effective in improving lipid profiles, reducing total cholesterol, LDL and triglyceride levels and boosting suboptimal HDL. In other research, skipping breakfast is linked with higher rates of cardiovascular disease, including a significantly heightened risk of cardiovascular mortality. One study suggests skipping breakfast while eating late at night can increase the likelihood of coronary heart disease by 55 percent, and another study found overeating low-quality carbs and animal protein at dinner rather than breakfast was significantly correlated with higher cardiovascular disease risk.8, 9, 10, 11, 12
Relaxation: yoga, meditation and stress reduction.
The relationship between emotional stress and cardiovascular risk factors is well established. Heightened stress is connected with higher inflammation, elevated heart rate and blood pressure, and a higher likelihood of cardiovascular events. Stress also triggers heightened sympathetic activity which impacts lipid metabolism, and studies link increased emotional stress with higher total cholesterol and LDL and lower HDL. Relaxation practices like meditation not only decrease heart rate and blood pressure but also normalize stress hormones, reduce inflammation and improve lipid profiles. Sympathetic nervous system overactivity is implicated in elevated cholesterol independent of diet. By blunting sympathetic activation, meditation can lower total cholesterol and triglycerides. In one meta-analysis, people engaged in regular meditation showed significant reductions in cholesterol levels compared to non-meditators, as well as favorable and even more pronounced impacts on triglycerides. In addition to static meditation practices, yoga not only decreased stress and blood pressure and other cardiometabolic risk factors, but also balanced lipid profiles. One review found movement-based meditation techniques like yoga were associated with significantly reduced total cholesterol and triglyceride levels. Similar effects have been seen in qigong.13, 14, 15, 16, 17
Exercise: aerobics, endurance training and HIIT.
Besides improving cardiovascular function, slowing heart rate, lower blood pressure and inhibiting stress hormones, exercise also reduces LDL and triglycerides and increases HDL. The type of exercise is important: aerobic or endurance forms, like running, cycling, swimming, elliptical trainer, skiing or rowing, are shown to have most meaningful influence on blood lipids, raising HDL and decreasing total cholesterol, LDL and triglycerides. The greatest benefits are seen with moderate-intensity aerobic training 150 to 300 minutes a week, or 75 to 150 minutes a week for vigorous-intensity aerobic physical activity. Some studies suggest even 30 min of exercise per day may be sufficient to boost HDL.18, 19, 20, 21
In other research, high-intensity interval training (HIIT) was superior to moderate-intensity continuous training in decreasing LDL and total cholesterol. Compared to MICT, HIIT significantly lowered total cholesterol, as well as LDL concentrations. And where patients exercise may play a role: outdoor activities or exercising in the sunshine promotes vitamin D synthesis: studies link higher serum vitamin D levels with better cardiorespiratory fitness.22, 23
Red Yeast Rice: lipid-lowering stain alternative.
Derived from Monascus purpureus yeast grown on white rice, red yeast rice is a powerful tool for supporting cardiovascular health and normalizing lipids. The process of fermentation yields a variety of bioactive compounds, including sterols, flavonoids, lignans, polysaccharides and monacolins and polyketides, shown to influence cholesterol synthesis. Monacolin K, the most abundant monacolin in red yeast rice, is chemically similar to the cholesterol-lowering drug lovastatin and clinical trials demonstrate its ability to benefit lipid levels, even at low doses.24, 25, 26, 27, 28
In numerous systematic reviews, red yeast rice supported healthy LDL and HDL, total cholesterol and triglycerides, with greater effects on patients with dyslipidemia. Red yeast rice also decreased ApoB, while slowing inflammation, stabilizing vulnerable atherosclerotic plaque and improving markers of arterial health. Other research shows significant reductions in the risk for mortality and major coronary events. Because it’s safe and well-tolerated in people intolerant to standard lipid therapy, red yeast rice offers a valuable alternative.29, 30, 31, 32, 33, 34, 35
Phytosterols: anti-inflammatory complement to cholesterol drugs.
Naturally occurring in plant sources like vegetable oils, almonds, wheat germ and wheat bran, phytosterols have proven antioxidant, anti-inflammatory and lipid-lowering properties. B-sitosterol, campesterol, stigmasterol and other phytosterols are structurally similar to cholesterol, thus competing with dietary cholesterol for absorption. Unlike cholesterol, sterols are primarily pumped back into the intestinal lumen, and less than one percent of sterols are ultimately retained. Along with inhibiting intestinal absorption of dietary cholesterol, phytosterols also affect cholesterol metabolism, increasing its excretion and reducing the synthesis of VLDLs.36, 37, 38, 39, 40
In dozens of studies, phytosterol treatment is correlated with significant decreases in LDL, total cholesterol and triglycerides, with some research showing 2 to 3 grams per day lowered LDL by 6 to 12 percent and triglycerides by 6 to 9 percent, with no significant effect on HDL. Phytosterol supplementation was also associated with reductions in ApoB, ApoE and the ApoB/ApoA-I ratio, as well as an increase in ApoA-I. Used in conjunction with standard lipid therapies, phytosterols further decrease total cholesterol and LDL, and when combined with red yeast rice, enhance the reductions of LDL and ApoB.41, 42, 43
Garlic: wide-ranging cardioprotective benefits.
Well-known for its cardioprotective properties, garlic is rich in bioactive compounds, including alliin, allicin, S-allyl cysteine and diallyl trisulfide, shown to work through a variety of mechanisms, normalizing blood pressure, slowing inflammation, suppressing clot formation and protecting against atherosclerosis, and supporting healthy lipid profiles. Studies link garlic supplementation with significant reductions in C-reactive protein and TNF-α, and dozens of trials validate its efficacy in promoting normal LDL and total cholesterol levels. Garlic influences dietary cholesterol absorption and cholesterol synthesis, and one meta-analysis found that garlic supplementation reduced total cholesterol and LDL. In another meta-analysis, garlic supplementation lowered total cholesterol, LDL and triglycerides, and improved blood pressure, waist circumference and BMI. In people with coronary artery disease, garlic supplementation significantly decreased total cholesterol and LDL, increased HDL, minimized inflammation and improved coronary artery calcium scores.44, 45, 46, 47, 48, 49
Aged garlic extract (AGE) appears to be especially cardioprotective. In one trial, AGE inhibited coronary artery calcium progression, while reducing inflammation, blood pressure and blood glucose in patients at higher risk for cardiovascular events. Another study found AGE significantly decrease systolic and diastolic blood pressure and improved central blood pressure and pulse wave velocity in patients with uncontrolled hypertension. In a systematic review of trials evaluating the efficacy of interventions on cardiovascular calcification, only AGE consistently showed benefit.50, 51, 52
Berberine: traditional, plant-based lipid balance.
An isoquinoline alkaloid found in barberry, goldenseal and other plants, berberine has been used for centuries in traditional medicine. Current evidence validates its cardioprotective effects, with studies demonstrating its antioxidant and anti-inflammatory properties: research suggests berberine enhances the activity of antioxidant enzymes, regulates the production of cytokines and suppresses inflammatory responses. Berberine improves additional aspects of cardiovascular health, including blood pressure, BMI and glucose metabolism, attributed in part to its influence on gut microbiota composition and diversity. Berberine has also been shown to support healthy lipid profiles, decreasing LDL, triglycerides and ApoB, while increasing HDL.53, 54, 55, 56
In one study, 500 mg of berberine twice a day had significant effects on lipids, including a 29 percent reduction in total cholesterol, a 25 percent reduction in LDL and a 35 percent reduction in triglycerides. In another study, 500 mg of berberine twice daily lowered LDL by an average of 23.8 percent. Berberine appears to impact lipids through different mechanisms than those of red yeast rice or statins. It’s thought to upregulate the expression of LDL receptors and suppress the expression of PCSK9. Because it works primarily by inhibiting PCSK9, berberine may also enhance the effectiveness of red yeast rice, as well as standard lipid-lowering drugs. In one study, a combination of simvastatin and berberine decreased LDL by an average of 31.8 percent, and other research suggests berberine is a viable alternative for patients who are intolerant to statins.57, 58, 59, 60, 61, 62
References:
- Dyńka D et al. The Ketogenic Diet and Cardiovascular Diseases. Nutrients. 2023 Jul 28;15(15):3368.
- Ma D et al. Ketogenic diet enhances neurovascular function with altered gut microbiome in young healthy mice. Sci Rep. 2018;8:6670.
- Tang WH et al. Gut Microbiota in Cardiovascular Health and Disease. Circ Res. 2017 Mar 31;120(7):1183-1196.
- Li C et al. Gut microbiome and metabolome profiling in Framingham heart study reveals cholesterol-metabolizing bacteria. Cell. 2024 Mar 21:S0092-8674(24)00305-2.
- Al Samarraie A et al. Role of the Gut Microbiome in the Development of Atherosclerotic Cardiovascular Disease. Int J Mol Sci.2023; 24, 5420.
- Attaye I et al.The Role of the Gut Microbiota on the Beneficial Effects of Ketogenic Diets. Nutrients. 2021 Dec 31;14(1):191.
- Khan I et al. Exploring blood microbial communities and their influence on human cardiovascular disease. J Clin Lab Anal. 2022 Apr;36(4):e24354.
- Ahmed N et al. Impact of Intermittent Fasting on Lipid Profile-A Quasi-Randomized Clinical Trial. Front Nutr. 2021 Feb 1;7:596787.
- Deshmukh-Taskar P et al. The relationship of breakfast skipping and type of breakfast consumed with overweight/obesity, abdominal obesity, other cardiometabolic risk factors and the metabolic syndrome in young adults. The National Health and Nutrition Examination Survey (NHANES): 1999-2006. Public Health Nutr. 2013 Nov;16(11):2073-82
- Rong S et al. Association of Skipping Breakfast With Cardiovascular and All-Cause Mortality. J Am Coll Cardiol. 2019 Apr 30;73(16):2025-2032.
- Cahill LE et al. Prospective study of breakfast eating and incident coronary heart disease in a cohort of male US health professionals. Circulation. 2013 Jul 23;128(4):337-43.
- Hou W et al. Meal Timing of Subtypes of Macronutrients Consumption With Cardiovascular Diseases: NHANES, 2003 to 2016. J Clin Endocrinol Metab. 2021 Jun 16;106(7):e2480-e2490.
- Schneider RH, Carr T. Transcendental Meditation in the prevention and treatment of cardiovascular disease and pathophysiological mechanisms: An evidence-based review. Adv Integr Med. 2014 Dec;1(3):107-112.
- Barnes VA, Orme-Johnson DW. Clinical and Pre-clinical Applications of the Transcendental Meditation Program in the Prevention and Treatment of Essential Hypertension and Cardiovascular Disease in Youth and Adults. Curr Hypertens Rev. 2006 Aug 1;2(3):207-218.
- Antonelli M et al. Effects of Static Meditation Practice on Blood Lipid Levels: A Systematic Review and Meta-Analysis. Healthcare (Basel). 2024 Mar 14;12(6):655.
- Isayeva AS et al. Blood lipids and anthropometric parameters in healthy subjects practicing yoga or resistance training in leisure time. What matters: type or intensity of physical activity?Pol Merkur Lekarski.(2021) 49:203–8
- Ghazvineh D et al. The Effect of Yoga on the Lipid Profile: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Nutr. 2022;9:942702.
- Franczyk B et al. The Impact of Aerobic Exercise on HDL Quantity and Quality: A Narrative Review. Int J Mol Sci. 2023 Feb 28;24(5):4653.
- Harrison M et al. Lipoprotein particle distribution and skeletal muscle lipoprotein lipase activity after acute exercise. Lipids Health Dis. 2012;11:64.
- Zhao S et al. Effects of aerobic exercise on TC, HDL-C, LDL-C and TG in patients with hyperlipidemia: A protocol of systematic review and meta-analysis. 2021;100:e25103.
- Argani N et al. Comparison of the effect of different intensity exercise on a bicycle ergometer on postprandial lipidemia in type II diabetic patients. ARYA Atheroscler. 2014;10:147
- McCormick CP et al. The Effects of HIIT vs. MICT and Sedentary Controls on Blood Lipid Concentrations in Nondiabetic Overweight and Obese Young Adults: A Meta-analysis. Int J Exerc Sci. 2023 Jun 1;16(3):791-813.
- Marawan A et al. Association between serum vitamin D levels and cardiorespiratory fitness in the adult population of the USA. Eur J Prev Cardiol. 2019 May;26(7):750-755.
- Cicero AFG et al. Red Yeast Rice for Hypercholesterolemia. Methodist Debakey Cardiovasc J. 2019 Jul-Sep;15(3):192-199.
- Heinz T et al. Low daily dose of 3 mg monacolin K from RYR reduces the concentration of LDL-C in a randomized, placebo-controlled intervention. Nutr Res. 2016; 36(10), 1162–1170.
- Benjian C et al. Effectiveness and safety of red yeast rice predominated by monacolin K β-hydroxy acid form for hyperlipidemia treatment and management. J Tradit Chin Med. 2022 Apr;42(2):264-271.
- Cicero AFG et al. Red Yeast Rice for the Improvement of Lipid Profiles in Mild-to-Moderate Hypercholesterolemia: A Narrative Review. Nutrients. 2023; 15(10), 2288.
- Rahmani P et al. Impact of red yeast rice supplementation on lipid profile: a systematic review and meta-analysis of randomized-controlled trials. Expert Rev Clin Pharmacol. 2023 Jan;16(1):73-81.
- Li P et al. Red Yeast Rice for Hyperlipidemia: A Meta-Analysis of 15 High-Quality Randomized Controlled Trials. Front Pharmacol. 2022; 12, 819482.
- Cicero AF et al. Red yeast rice improves lipid pattern, high-sensitivity C-reactive protein, and vascular remodeling parameters in moderately hypercholesterolemic Italian subjects. Nutr Res. 2013 Aug;33(8):622-8.
- Yuan R et al. Red Yeast Rice Preparations Reduce Mortality, Major Cardiovascular Adverse Events, and Risk Factors for Metabolic Syndrome: A Systematic Review and Meta-analysis. Front Pharmacol. 2022; 13, 744928.
- Lu Z et al. Effect of Xuezhikang, an extract from red yeast Chinese rice, on coronary events in a Chinese population with previous myocardial infarction. Am J Cardiol. 2008; 101(12), 1689–1693.
- Halber SC et al. Tolerability of red yeast rice (2,400 mg twice daily) versus pravastatin (20 mg twice daily) in patients with previous statin intolerance. Am J Cardiol. 2010 Jan 15;105(2):198-204.
- Banach M et al. The Role of Nutraceuticals in Statin Intolerant Patients. J Am Coll Cardiol. 2018 Jul 3;72(1):96-118.
- Xue Y et al. Red yeast rice induces less muscle fatigue symptom than simvastatin in dyslipidemic patients: a single center randomized pilot trial. BMC Cardiovasc Disord. 2017;17(1), 127.
- Cabral CE, Klein MRST. Phytosterols in the Treatment of Hypercholesterolemia and Prevention of Cardiovascular Diseases. Arq Bras Cardiol. 2017 Nov;109(5):475-482.
- Javanmardi MA et al. Effects of Phytosterol Supplementation on Serum Levels of Lipid Profiles, Liver Enzymes, Inflammatory Markers, Adiponectin, and Leptin in Patients Affected by Nonalcoholic Fatty Liver Disease: A Double-Blind, Placebo-Controlled, Randomized Clinical Trial. J Am Coll Nutr. 2018 May 16:1-8.
- Davis HR et al. Niemann-Pick C1 Like 1 (NPC1L1) is the intestinal phytosterol and cholesterol transporter and a key modulator of whole-body cholesterol homeostasis. J Bio Chem. 2004; 279(32), 33586–33592.
- Makhmudova U et al. Phytosterols and Cardiovascular Disease. Current Atherosclerosis Reports. 2021; 23(11), 68.
- Li X et al. The Bioavailability and Biological Activities of Phytosterols as Modulators of Cholesterol Metabolism. Molecules. 2022 Jan 14;27(2):523.
- Ghaedi E et al. Phytosterol Supplementation Could Improve Atherogenic and Anti-Atherogenic Apolipoproteins: A Systematic Review and Dose-Response MetaAnalysis of Randomized Controlled Trials. J Am Coll Nutr. 2020 Jan;39(1):82-92.
- Malina DM et al. Additive effects of plant sterols supplementation in addition to different lipid-lowering regimens. J of Clin Lipidol. 2015; 9(4), 542–552.
- Cicero AFG et al. Effect of a short-term dietary supplementation with phytosterols, red yeast rice or both on lipid pattern in moderately hypercholesterolemic subjects: a three-arm, double-blind, randomized clinical trial. Nutr Metab (Lond). 2017 Sep 25;14:61.
- Li M et al. Roles and mechanisms of garlic and its extracts on atherosclerosis: A review. Front Pharmacol. 2022; 13, 954938.
- Sahebkar A et al. Lipid-modifying effects of nutraceuticals: An evidence-based approach. Nutrition. 2016; 32(11-12), 1179–1192.
- Ried K et al. Effect of garlic on serum lipids: an updated meta-analysis. Nutrition Reviews. 2013; 71(5), 282–299.
- Sun YE et al. Anti-hyperlipidemia of garlic by reducing the level of total cholesterol and low-density lipoprotein: A meta-analysis. Medicine. 2018; 97(18), e0255.
- Fu Z et al. Effects of garlic supplementation on components of metabolic syndrome: a systematic review, meta-analysis, and meta-regression of randomized controlled trials. BMC Complementary Medicine and Therapies. 2023; 23(1), 260.
- Gadidala SK et al. Effect of garlic extract on markers of lipid metabolism and inflammation in coronary artery disease (CAD) patients: A systematic review and meta-analysis. Phytotherapy Research. 2023; 37(6), 2242–2254.
- Wlosinska M et al. The effect of aged garlic extract on the atherosclerotic process – a randomized double-blind placebo-controlled trial. BMC Complement Med Ther. 2020 Apr 29;20(1):132.
- Ried K et al. The effect of aged garlic extract on blood pressure and other cardiovascular risk factors in uncontrolled hypertensives: the AGE at Heart trial. Integr Blood Press Control. 2016 Jan 27;9:9-21.
- Murali S et al. Interventions to Attenuate Cardiovascular Calcification Progression: A Systematic Review of Randomized Clinical Trials. J Am Heart Assoc. 2023 Dec 5;12(23):e031676.
- Zamani M et al. The effects of berberine supplementation on cardiovascular risk factors in adults: A systematic review and dose-response meta-analysis. Front Nutr. 2022 Oct 14;9:1013055.
- [1] Zhang Y et al. Gut Microbiome-Related Effects Of Berberine And Probiotics On Type 2 Diabetes (The PREMOTE Study). Nat Comm. 2020; 11(1), 5015.
- Blais JE et al. Overall and Sex-Specific Effect of Berberine for the Treatment of Dyslipidemia in Adults: A Systematic Review and Meta-Analysis of Randomized Placebo-Controlled Trials. Drugs. 2023; 83(5), 403–427.
- Ju J et al. Efficacy and safety of berberine for dyslipidaemias: A systematic review and meta-analysis of randomized clinical trials. Phytomedicine. 2018 Nov 15;50:25-34.
- Koppen LM et al. Efficacy of Berberine Alone and in Combination for the Treatment of Hyperlipidemia: A Systematic Review. J Evid Based Complementary Altern Med. 2017 Oct;22(4):956-968.
- Yin J et al. Traditional chinese medicine in treatment of metabolic syndrome. Endocr Metab Immune Disord Drug Targets. 2008 Jun;8(2):99-111.
- Zhang LS et al. Efficacy and Safety of Berberine Alone or Combined with Statins for the Treatment of Hyperlipidemia: A Systematic Review and Meta-Analysis of Randomized Controlled Clinical Trials. Am J Chin Med. 2019; 47(4), 751–767.
- Pisciotta L et al. Nutraceutical pill containing berberine versus ezetimibe on plasma lipid pattern in hypercholesterolemic subjects and its additive effect in patients with familial hypercholesterolemia on stable cholesterol-lowering treatment. Lipids Health Dis. 2012; 11, 123.
- Li H et al. Hepatocyte nuclear factor 1alpha plays a critical role in PCSK9 gene transcription and regulation by the natural hypocholesterolemic compound berberine. J Bio Chem. 2009; 284(42), 28885–28895.
- Kong WJ et al. Combination of simvastatin with berberine improves the lipid-lowering efficacy. Metabolism. 2008;57:1029–1037.